In the following pages, my goal is to help you get a functional understanding of Medicare Advantage (MA) Star ratings, primarily what they are, what they are composed of, and a glimpse on why they are important for payors and consumers. In future editions, I will plan on getting into the weeds on trends in the stars ratings, as well as into how they get calculated.
Executive Summary
- There are multiple variations of stars ratings that are published by CMS, here we will dig into the stars ratings that evaluate Medicare Advantage plans. Each year, Medicare Advantage plans are evaluated and assigned a star rating from 1 to 5 stars, where 5 is excellent.
- Star measures are composed of data from quality measures (HEDIS), patient experience data (CAHPS), third-party reviews, and other administrative data sources within CMS.
- The star rating is a way for consumers to easily evaluate the quality and performance of Medicare advantage plans.
- High performing plans may be eligible for additional bonuses, able to market themselves as high performers, or be open to year round open-enrollment in case of achieving the coveted 5 star rating.
Medicare Advantage may refer to a few different types of plans:
- Medicare Advantage only (supplementary to traditional A & B) sometimes referred to as Part-C.
- Medicare Advantage part D (above + prescription drug benefits)
- Prescription Drug Plans (no supplemental coverage to A & B, only prescription drug benefits).
What’s a Star Rating?
Beginning in the late 2000s, star ratings began to appear to help consumers evaluate quality and performance of Medicare advantage plans they may be shopping for. All established Medicare advantage plans come with a star rating, with 1 being lowest and 5 being highest.
These star measures are composed of summary scores, domain scores, and up to 42 different measures (in 2024) that evaluate clinical care quality, patient experience, medication adherence, and other administrative processes. By converting these measures into star ratings, users can more readily compare performance of MA plans as opposed to wading through dozens of raw measures.
Current star ratings for all Medicare advantage plans can be found here on Medicare.gov. In the appendix, I walk through a real-life example of what they look like in practice.
Why Do Stars Matter?
Healthcare has long been working to transition to a value based care framework that rewards high quality and low cost of care. Through the assignment of star ratings we can start to see high quality represent itself between payors.
For payors:
- Plans are able to market themselves against other plans to drive higher enrollment volumes.
- As long as plans keep costs below an established benchmark set by CMS, they may be eligible for bonus payments of up to 5% should their star rating be 4 or greater [3].
- Plans that attain a 5 star rating are able to enroll patients year round as opposed to the enrollment period that occurs at the end of each year.
- Consistently low performers (less than 3 stars) may be terminated from selling/offering plans.
For Consumers:
- Simplifying scores into a star rating can be much more digestible as each of the star ratings consist of multiple measures that may be in form of percentages or values, where some have low-values = good, and others have high values = good.
- Consumers are also more likely to enroll in plans that have higher star ratings.
Consumers tend to purchase from plans that are 4+ stars or greater
% of Total Medicare Advantage Contracts vs Total Members in 2024
Criticisms and Feedback
- One significant criticism of star ratings is that they do not entirely incentivize health equity among members. Contracts may receive a boost in their star ratings if a certain percentage of their members is composed of large volumes of low-income, disabled, or dual-eligibles (people eligible for Medicare & Medicaid). However, plans are not necessarily incentivized to address health disparities outside of the above factors. Beginning in 2027, CMS is planning on adding a reward factor to plans that outperform others when addressing specific social risk factors (SRFs) [1].
- Changes in methodology have also come under criticism (mainly from payors). For example, in 2024 CMS implemented a new statistical methodology, the Tukey Outer Fence Outlier Deletion Method, which removes extreme outliers in the data before applying a star rating. Since the majority of these outliers were on the lower end, it increases the average (and cut-points) in various measures making it harder to attain 4 and 5 star ratings. While some may argue this is important from a mathematical perspective, it also means less plans will be eligible for bonus payments, with some estimates to be around $800 million [2] less in bonus payments.
- Critics also argue that the measures place an over emphasis on patient reported experiences rather than quality of care. While care delivery measures make up over half of the total measures, they are not weighted as heavily as patient experience measures (see table 2 for breakdown)
Breaking Down Star Ratings
Let’s get back to understanding stars and how they are put together. Within a plan’s star ratings there are four distinct scores, all of which are rated from 1 to 5 stars.
Overall Plan Score
This is the first rating that an individual may see when shopping for plans and represents the plan’s overall score.
Summary Score
There are two possible summary scores, a health plan score and a drug plan score:
- Plans offering only Medicare Advantage (MA) will have a health plan score only
- Plans offering Medicare Advantage in addition to drug coverage (MA-PD), will have both a health plan and a drug plan score.
- Plans offering only prescription drug plans (PDP) coverage will have a drug plan score.
Domain Scores
Domain scores represent buckets of like measures covering care delivery processes and outcomes, along with member experience. Each domain may be composed of 1 to to 14 measures (see Table 2 for more below)
Measures
- Measures are the raw processes or outcomes being evaluated. Each measure in its raw format is a numeric or percentage value that is converted into a specific star rating based on performance compared to peers. This segmentation is done through a statistical approach called clustering (covered in a future article) which establishes cut points for each star rating and differs between measures.
- Cut points are not known ahead of time, which incentivizes plans to continuously improve their operations. Cut points for the current year are published by CMS.
- Data for measures comes from a variety of sources including HEDIS measures that evaluate quality of care, CAHPS survey data to evaluate patient experience, and other administrative sources from both the plans and CMS [see Table 1]
Table 1. Summary of Data Sources for Measures
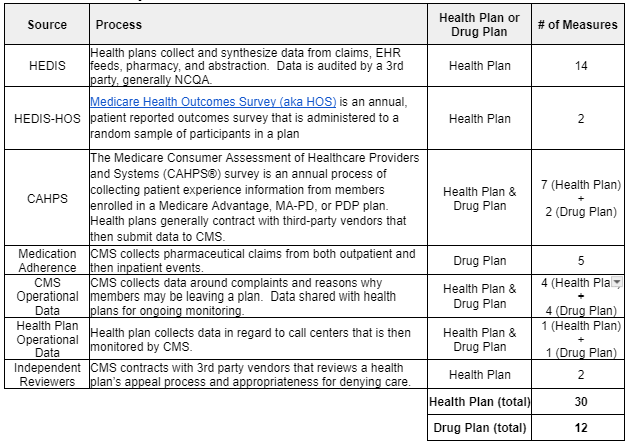
- Plans must report on all measures for their given plan. In cases where plans are too new to have data or don’t meet a minimum enrollment volume, measures will be displayed as such.
- CMS may opt to change measures from year-to-year as it deems appropriate based on goals of the program or feedback from plans.
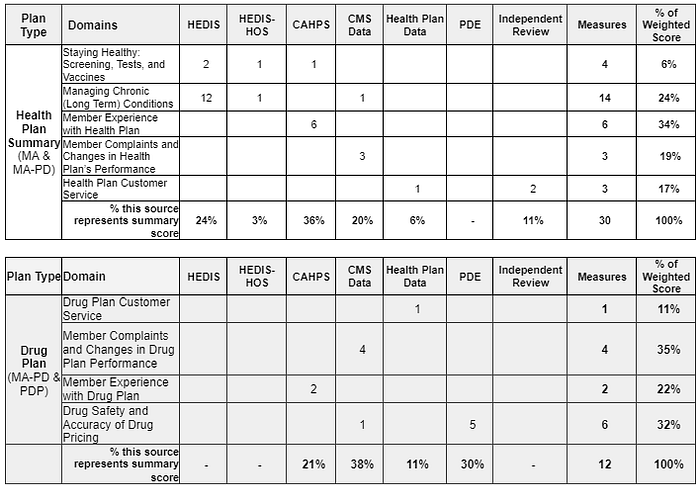
- Measures are given a weighting, making some more impactful to final scores than others. Process measures are generally weighted as a 1, outcomes are weighted as 3, and patient experience and complaints are weighted as a 4, while improvement is rated a 5 [Table 2].
Table 2. Breakdown of Where measures Are Sourced from and Their Impacts on Summary Scores
From Raw Measure to Overall Score
The overall, summary, and domain scores are calculated by pooling all appropriate measures together versus rolling each up in a hierarchical manner. In other words, for a Medicare Advantage Part-D plan:
- The 9 domain scores may have anywhere from 1–14 measures (see table 2)
- Summary for Health Plan performance has 30 measures.
- Summary of Drug Plan performance has 12 measures.
- Overall summary is composed of all 42 measures.
Below you can see a framework of how these measures are rolled up. Note that the individual measures are responsible for driving scores at each level. They are not rolled up from measure to domain, to plan, to summary.
Stars Publishing Timeline
The process of collecting, validating, and submitting data from all these sources is an arduous and timely process. Because of this, the current stars ratings reflect measures that are from data that may be over a year old. Given open enrollment for consumers begins late in Q4 of each year, there is a need to collect, process, and validate data. Because of this, data can be several months old by the time consumers first see ratings. This timeline can be found in figure 3 below.
Figure 3. Approximate timeline for 2024 Stars rating publication.
Summary
In sum, Medicare Advantage star ratings are composed of dozens of measures and rolled up in a manner that is supposed to help consumers understand the quality and performance of health or drug plans they may be enrolling in. For payors, it is an opportunity to focus on quality initiatives within their plan and care delivery partners such that they may be rewarded financially, either through increased enrollment or bonus payments from Medicare.
In future iterations, I hope to dive into overall quality trends to see if plans are truly increasing in quality over time, as well as open up the black box on how CMS transforms raw measure scores into a unique star rating.
Sourcing Notes:
[1] https://www.healthmine.com/resources/health-equity-index-star-ratings-impact
[2] https://www.chartis.com/insights/medicare-advantage-2024-star-ratings-more-stars-fade-again-year
[3] https://www.urban.org/research/publication/medicare-advantage-quality-bonus-program
Appendix
Examples Captured from Medicare.Gov
To see how this looks in practice, let’s take a look at real-life examples (if you’d like to explore on your own, you can do so on Medicare.gov).
Here is a plan that I found near me (note that this is a Medicare Advantage only option)
When we explore the star summary (at bottom of the page), we can see both the overall rating, as well as the ratings for the domains. (Note that the raw scores for these are not marketed, only the star ratings). Here we continue to see the overall star rating (orange), followed by the summary ratings (purple).
Medicare Advantage Only Plan
Medicare Advantage Part D Plan
Expanding further, we can also explore the domains of one of these plans. Here I drill into a health plan star rating and can see the individual domains starting with “Staying Healthy: Screening, Tests, & Vaccines”
Finally, we can observe the star ratings for individual measures that make up each of the domains. Here we can see the staying healthy domain and the associated preventative measures that make up the rating (breast cancer screening, followed by colorectal cancer screening, etc.)
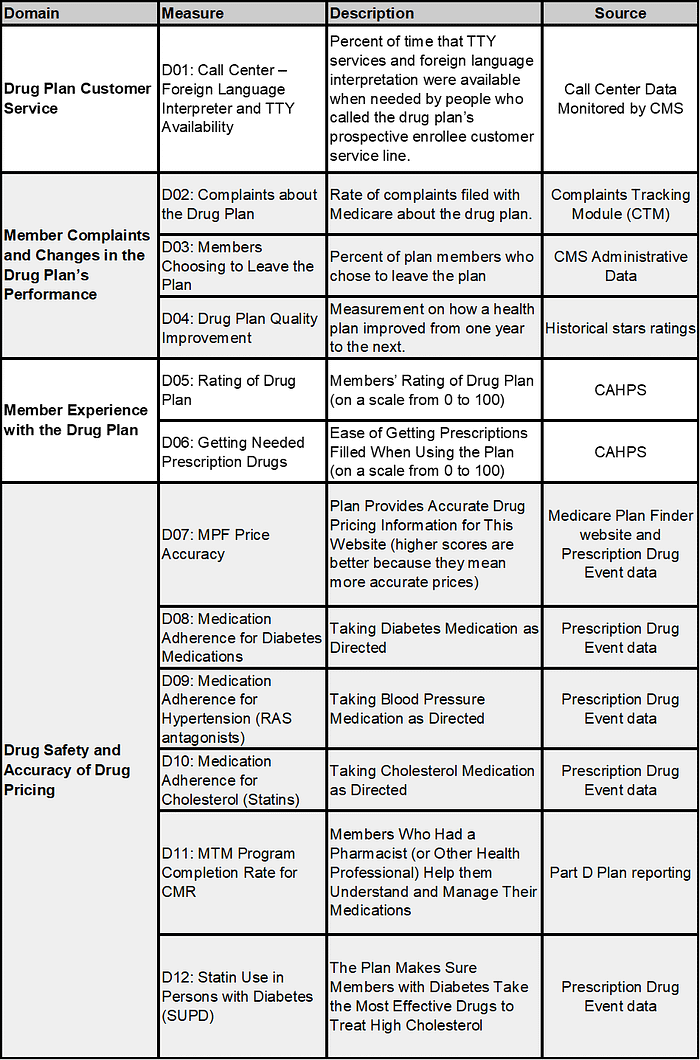
Measures Reported in 2024 Medicare Advantage Star Ratings
Below is a summary of all measures captured in the 2024 Medicare Advantage Star ratings. For a more comprehensive listing with definitions, data sourcing, weights, etc. Please review the 2024 technical notes found on CMS’ website here: https://www.cms.gov/medicare/health-drug-plans/part-c-d-performance-data
Table 3 — Health Plan Rating (MA-only & MA-PD)
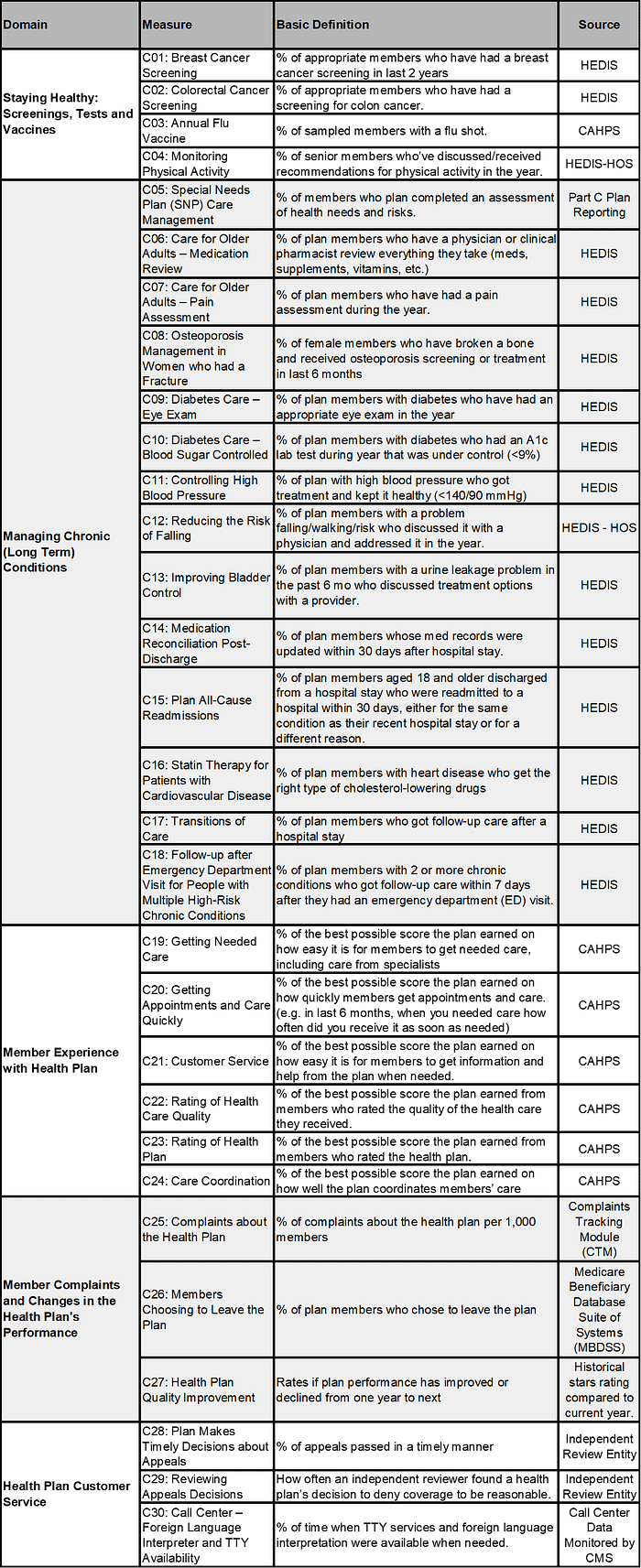
Table 4 — Drug Plan Rating (MA-PD & PDP)